Introduction
Odontogenic tumours are infrequent lesions. It constitute approximately 0.002 - 0.003% of all the body tumours.[1] The biological behavior of these tumours inclu¬de hamartomatous proliferation, non-aggressive benign tumours, and aggressive and malignant tumors.[2] There has been considerable interest in odontogenic tumours by oral pathologists, who have studied and catalogued these tumours for decades.[3]
Studies on odontogenic tumours published from many parts of the world show a distinct geographic variation in relative prevalence.[1],[4],[5],[6] But there is little information available in the literature on the relative frequency of odontogenic tumours in India.
The present study was carried out to establish the prevalence of odontogenic tumours in Puducherry, South India, and to compare the basic clinical features derived from this study with that of WHO figures.
Materials and Methods
Histopathological records of odontogenic tumours were retrieved from the Department of Oral Pathology and Microbiology, Mahatma Gandhi Post Graduate Institute of dental sciences, Puducherry. Data was collected from 1999 -2008. Total numbers of the biopsied specimen were counted in the last decade. Out of them histopathologically diagnosed odontogenic tumours were noted down. The variables gender, age, anato¬mical site, histological type and symptoms were analyzed in the histopathology reports.
These were classified according to WHO 2005 histopathological classification.[7] Total percentage of odontogenic tumours, with individual odontogenic tumour percentages was calculated. All these clinical data were then compared with WHO figures.
Results
Total number of surgical specimen received by the department of oral pathology and microbiology was 1883. Out of which 61 were odontogenic tumors inclusive of odontogenic keratocysts. Total percentage of odontogenic tumors was 3%. Out of these tumors 97% were benign and 3% were malignant. Keratocystic odontogenic tumour was the most common odontogenic tumour (37%). It was followed by Ameloblastoma (26%) and then by Calcifying epithelial odontogenic tumour and Adenomatoid odontogenic tumor (10%). Odontogenic tumors were more common in 2nd to 4th decade of life. Odontogenic tumours had shown female predilection in our study.
Discussion
Odontogenic tumour constitute a very small percentage of whole body tumours (.002%-.003%).[1] But these lesions occupy a very important place in tumors of jaw bones. Maximum available studies in the past were based on WHO 1992 histopathological classification. Few changes were done in WHO 2005 classification.[7] Out of them one of very important change was inclusion of keratocystic odontogenic tumor as a benign neoplasm.[3]
According to previous studies which has followed WHO 1992 classification Ameloblastoma was the most prevalent tumour with different prevalence in different parts of world. Total percentage of odontogenic tumours in this study was 3% of the entire specimen received in the department of oral pathology, this is little higher than study done by Alevar et al[3] (2.5%). According to study done by Regezi et al[5], the odontogenic tumours constitute <2-3% of all the specimen received in the department of oral pathology. In the present study 97% of the odontogenic tumors were benign and 3% were malignant. This data correlates with study done by Mosqueda T et al.[8] Most common tumour in this study was KCOT (37%) which is supported by study done by Avelar et al[3] and were contradictory to the study done by Jing W et al.[9] According to the present study there was a male predilection (2:1). It was same as WHO data but contradictory to studies done by Avelar et al.[3] The most common site for occurrence in the present study was posterior mandible. It is in accordance with the WHO data.
In our study ameloblastoma was the second most common tumour (26%), where as in a study done in India by Sriram et al[10] ameloblastoma was found to be the most common tumour (61.5%). This tumour had shown female predilection in our study. But WHO data shows more predilections for male gender. Our study was supported by studies done in Hong Kong[11] and Michigan[5]. Anatomical site and age prevalence were same as WHO figures.
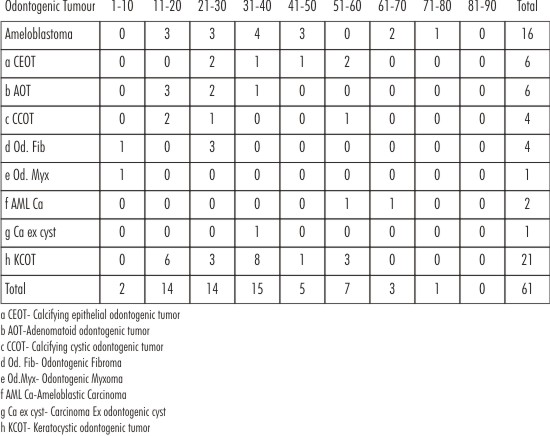 | Table - I Age (in Years) distribution of odontogenic tumors
 |
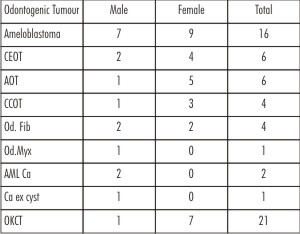 | Table II- Gender distribution of various odontogenic tumors
|
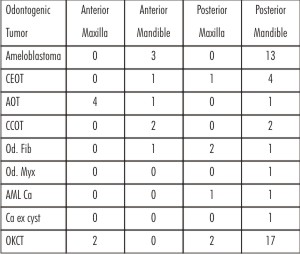 | Table III-Site predilection of odontogenic tumours
|
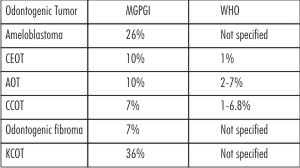 | Table IV-Comparison of frequency of odontogenic tumors with WHO figures
|
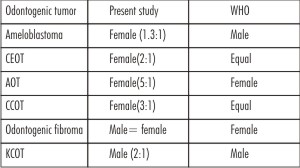 | Table V - Comparison of gender distribution between present study and WHO figures
|
 | Table VI - Comparison of site predilection of present study figures with WHO figures
|
 | Table VII- Comparison of Age distribution
|
Unexpectedly CEOT (10%) was the third most common tumour sharing place with AOT in the present study. According to WHO figure it constitutes just about 1%. In none of the studies in past, CEOT has emerged as one of the major tumour. This lesion has shown female preponderance in our study compared to WHO figures which shows equal predilection for both genders. AOT (10%) according to this study has got slightly more value than the WHO figures (2-7%). These figures were slightly less as compared to another Indian study (12%).[10] This lesion has shown a strong predilection for female gender and anterior maxilla and is supported by WHO figures and other studies.[3],[10],[12]
In the present study CCOT constituted 7% of all odontogenic tumour and falls in the range given by WHO (1-6.8%). This lesion have also shown female predilection whereas WHO figures show equal gender distribution. It was found to be more common in posterior mandible in this study. But WHO data shows same predilection for both jaws (cuspid region).
In this study odontogenic fibroma constituted 7% of all the odontogenic tumours with equal gender predilection. In other studies done in past this lesion never came up as a major tumour.[1],[2],[4],[5],[8],[13],[14] WHO shows more female predilection.
Studies done in western world [2],[8],[12] have shown odontogenic Myxoma as a major odontogenic tumour. But in the present study it shows lesser prevalence (1.6%).
Conclusion
Total percentage of odontogenic tumours were same as WHO figures. Odontogenic tumours are more common among females in Puducherry. KCOT was the most common tumour; CEOT and AOT were the second most common tumors. Age distribution is almost consistent with WHO figures. Ameloblastoma, CEOT and AOT are mostly site specific tumours. This epidemiological study is only an attempt to enlighten the prevalence of odontogenic tumours in southern part of India; which has got different geography and topography. Hence the difference in some data compared to WHO figures is logical to expect in this study.
Conflict of Interest - None declared
Acknowledgement - No funding was received for this study.
References
1. Gunhan O, Erseven G, Ruacan S, Celasun B, Aydinpug Y, Ergun E, Demiriz M. Odontogenic tumor: a study of 409 cases. Aust Dent J 1990; 35(6): 518-522.
2. Buchner A, Merrel PW, Carpenter WM. A relative frequency of central odontogenic tumors: A study of 1088 cases from northern California and comparison to the studies from other part of the world. J Oral Maxillofacial Surgery 2006 ; 64(9): 1343-1352.
3. Avelar RL, Antunes AA, Santos TS, Andrade ESS, Dourado E. Odontogenic tumors: clinical and pathology study of 238 cases. Rev Bras Otorrinolaringol 2008; 74(5): 668-673.
4. Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol 1994; 77(3): 276-280.
5. Regezi JA, Kerr DA, Courtney RM. Odontogenic tumors: analysis of 706 cases. J Oral Surg 1978; 36: 771-778.
6. Ladeinde AL, Ajayi OF, Ogunlewe MO, Adeyemo WL, Arotiba GT, Bamgbose BO et al. Odontogenic tumors: A review of 319 cases in a Nigerian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99(2): 191-195.
7. Barnes L, Everson J, Reichart P. World Health Organization Classifi¬cation of Tumours: Pathology and Genetics of Tumours of the Head and Neck. Lyon, France, International Agency for Research on Cancer, 2005.
8. Mosqueda Taylor A, Ledesma Montes C, Caballero sandobal S, Odontogenic tumor in mexico: A collaborative retrospective study of 349 cases. Triple O 1997; 84(6): 672-675.
9. JingW, Xuan M, Lin Y, WU L, Liu L, Xheng X, Tang W, Qiau J, Pian W. Odontogenic tumors :A retrospective study of 1642 cases in a Chinese population. Int J Oral Maxillofac Surg 2007; 36(1): 22-25.
10. Sriram G, Shetty RP. Odontogenic tumour: A study of 250 cases in an Indian teaching hospital. Oral Surg Oral Pathol Oral Radiol Endod 2006; 105: e14-21.
11. Wu P C, Chan K W. A survey of tumors of the jawbones in Hong Kong Chinese: 1963-1982. Br J Oral Maxillofac Surg 1985; 2(2): 92-102.
12. Santos JN, Pereira pinto, Sigueredo CRLVA, Desouza LB. Odontogenic tumours: Analysis of 127 cases. Pesqui Odontol Bras 2001; 15(4): 308-313.
13. Arotiba JT, Ogunbiyi JO,Obiechina AE. Odontogenic tumours: a 15 years review from Ibadan, Nigeria. British journal of oral & maxillofacial surgery 1997; 35: 363-367.
14. Ochsenius G, Ortega A, Godoy L, Peñafiel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases J Oral Pathol Med. 2002; 31(7):415-420. |